OSHA 301
This report provides the OSHA's Form 301 (Injury and Illness Incident Report). A report for each incident in the selected injury log is provided.
You can run this report from the Reports Directory or from the Injuries screen.
- . The report provides a list of only recordable records when run from this view.
- . The report provides a list of incidents regardless of the OSHA status when run from this view.
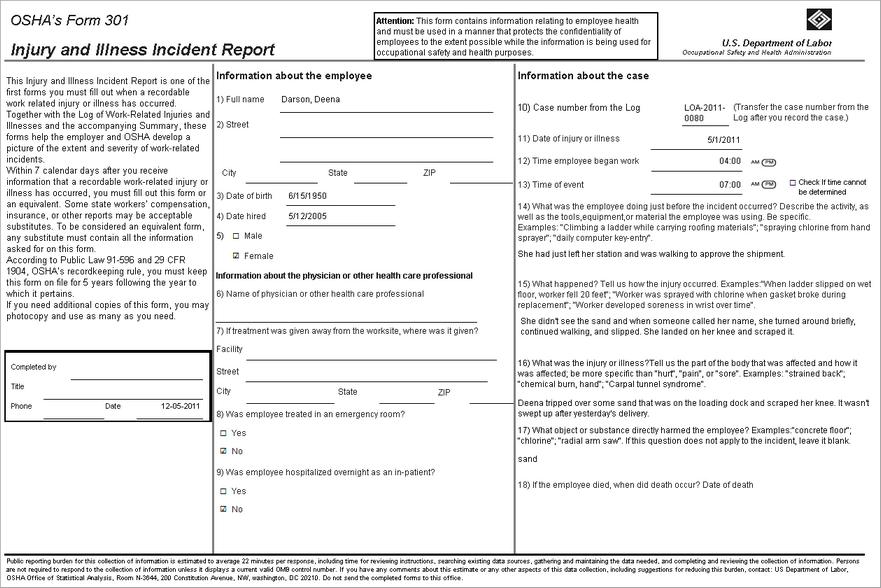
For privacy-cases, the system leaves both gender check boxes unchecked when you print the OSHA 301 report.
Report Parameters
| Parameter | Default Value | Details |
|---|---|---|
|
Date Range |
Month To Date |
Required |
|
Annual Average number of employees |
Blank |
Enter this figure based on your calculations, often calculated using the optional OSHA 300A worksheet. This field will print in the field of the same name on the Establishment Information section of the report. |
|
Total hours worked by all employees last year |
Blank |
Enter this figure based on your calculations, often calculated using the optional OSHA 300A worksheet. This field will print in the field of the same name on the Establishment Information section of the report. |
|
Injury Log ID |
None selected. |
Required. You can select a single Injury Log. |
The table below describes the OSHA 301 form fields and the corresponding PureSafety source fields. Go to or to view the source fields. The capitalized words in the PureSafety Source field column represent the tab on the Create Injury screen where the field displays.
| Form Field | LSMS Source Field |
|---|---|
|
Completed by |
Blank field to be entered at a later point manually. |
|
Title |
Blank field to be entered at a later point manually. |
|
Phone |
Blank field to be entered at a later point manually. |
|
Date |
Blank field to be entered at a later point manually. |
| Information about the employee | |
|
(1) Full Name |
EMPLOYEE: First Name, Middle Name, Last Name |
|
(2) Street Address |
EMPLOYEE: Address |
|
City |
EMPLOYEE: City |
|
State |
EMPLOYEE: State |
|
Zip |
EMPLOYEE: Zip |
|
(3) Date of birth |
EMPLOYEE: Birthday |
|
(4) Date hired |
EMPLOYEE: HIRE DATE |
|
(5) Male or Female |
EMPLOYEE: Gender |
| Information about the physician or other health care professional | |
|
(6) Name of physician or other health care professional |
TREATMENT: Name of Physician |
|
(7) If treatment was given away from the worksite, where was it given? |
|
|
Facility |
TREATMENT: Name of Medical Facility |
|
Street |
TREATMENT: Address |
|
City |
TREATMENT: City |
|
State |
TREATMENT: State |
|
ZIP |
TREATMENT: Zip |
|
(8) Was employee treated in an emergency room? |
TREATMENT: Emergency Room |
|
(9) Was employee hospitalized overnight as an in-patient? |
TREATMENT: Overnight |
| Information about the case | |
|
(10) Case number from the Log |
CASE: Case Number |
|
(11) Date of injury or illness |
INJURY: Injury Date |
|
(12) Time employee began work |
CASE: Time Began Work |
|
(13) Time of event |
INJURY: Injury Time |
|
(14) What was the employee doing just before the incident occurred? Describe the activity, as well as the tools, equipment, or material the employee was using. Be specific. |
INJURY: What was the employee doing just before the incident occurred? |
|
(15) What happened? Tell us how the injury occurred. |
INJURY: What Happened? |
|
(16) What was the injury or illness? Tell us the part of the body that was affected and how it was affected; be more specific than "hurt", "pain", or "sore". |
INJURY: Brief Description |
|
(17) What object or substance directly harmed the employee? If this question does not apply to the incident, leave it blank. |
INJURY: What object or substance directly harmed the employee? |
|
(18) If the employee died, when did the death occur? Date of Death |
INJURY: Date of Death |